Ryan Dugan, Nika Kazumyan, Julia Rothschild, Anika Sagar
Abstract
Approximately 10% of infants born in the US require respiratory support at birth. These apparatuses cause abrasions and pressure injuries. Our interface prototype, Ledernosen, aims to alleviate these pressure injuries, allowing less injurious long-term use of bubble CPAP (bCPAP) systems. We’ve focused on an adjustable suspension approach using wiring and flexible tubing. This allows for significant adjustment of the apparatus to improve fit on variable infant nasal geometries. We coupled this approach with a shock-absorbing prong shape, transferring pressure into the flexible silicone as opposed to the sensitive nasal tissue. We’ve verified our prototype through airflow testing coupled with computational fluid dynamics analysis. We found that our device delivers 92.3% ± 2.6% of input system airflow, without significant difference from the predicate Fisher & Paykel system delivery (p>0.5). We used contact pressure testing to determine the pressure exerted at the nares, and confirmed that our device exerted less pressure than the Fisher & Paykel interface under passive and active tension of the Flexi-TrunkTM (p<<<0.05).
Problem Statement
Current noninvasive respiratory support interfaces used to assist preterm neonatal breathing can cause extreme skin or tissue injury via excess friction and pressure. A reassessment of interface design that considers infant comfort is required to mitigate the risk of life-long facial disfigurement caused by necessary respiratory support.
Background
The cycle of care for bCPAP devices begins with a diagnosis of respiratory distress syndrome (RDS) [1]. RDS affects 90% of infants born at 24 weeks and 80% of those born at 28 weeks, typically presenting soon after delivery as decreased breath sounds, nasal flaring, lethargy, and cyanosis [1]. Preterm infants are especially prone to RDS due to the underdeveloped nature of their lungs [1]. Left untreated, RDS can progress to respiratory failure within 48-72 hours [1].
To support breathing, bCPAP provides constant positive pressure via humidity and temperature-controlled airflow. This pressure constantly assists breathing until the neonate is capable of independent respiration. BCPAP interfaces are available as nasal masks, prongs, and cannulas. Prolonged use of these interfaces creates pressure injuries because preterm neonate skin is fragile; therefore, these interfaces are alternated every 3-6 hours to offload pressure from regions of the neonate’s skin. Injury is further exacerbated by insufficient sizing or placement options to fit all nose anatomies comfortably. Frequent interventions and complicated sizing procedures can cause infant distress and compound the NICU nurses’ workload.
Reducing the prevalence and extremity of skin injury in neonates due to required respiratory support without sacrificing pressure delivery is a major unmet clinical need in NICUs.
Design Metrics
Based on literature values of pressure exerted by the Fisher & Paykel interfaces, and factors leading to infant injury, we determined the metrics in Table 1 as appropriate parameters for prototype performance evaluation:
| Feature | Target Values | Verification |
|---|---|---|
| Pressure Loss | <2.0 cmH2O | CFD |
| Nare Occlusion | ≥80% | Prong Dimensions |
| Nare Contact Pressure | 45 ± 15 mmHg |
Pressure testing on tissue-mimicking model |
| Forehead Contact Pressure | 50 ± 20 mmHg | Pressure-sensitive film |
| Placement Variation | <15% | Fit testing with nurses |
| Sizing Variation | <30% |
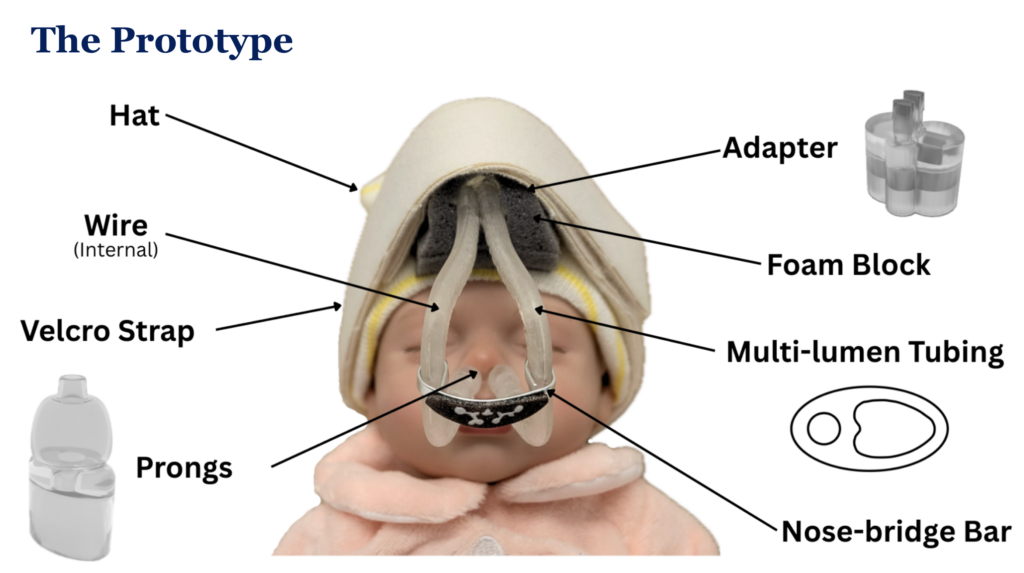
Prototype Construction
Modeling: CAD modeling was used for the prongs, tubing, and primary adapter.
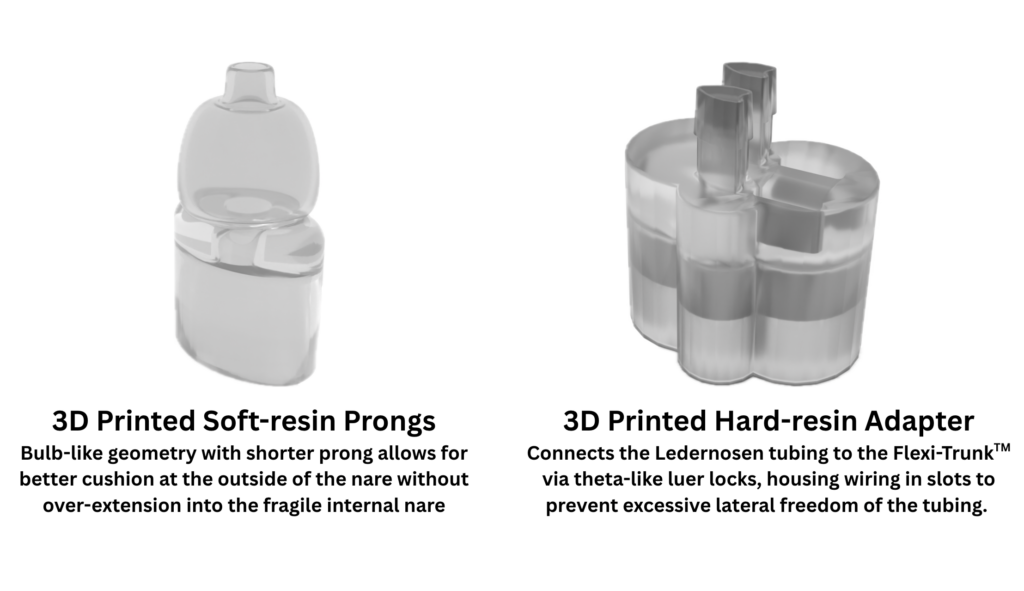
Resin 3D Printing: Used for high-speed printing of biocompatible elastic parts with intricate geometries.
Materials: The prongs and tubing were printed in biocompatible soft resin, whilst the tubing-Flexi-TrunkTM adapter was printed in biocompatible hard resin.
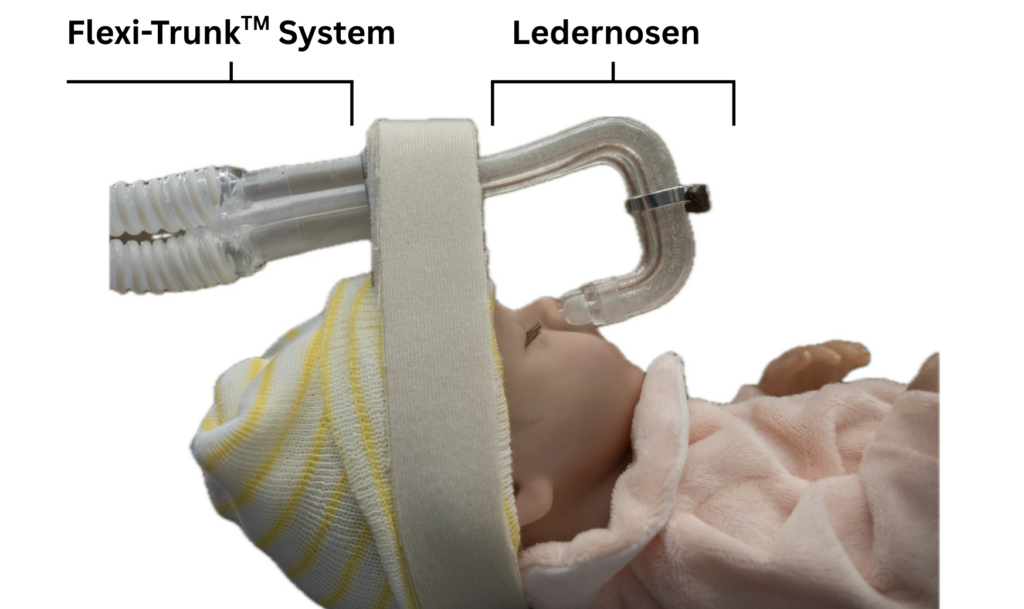
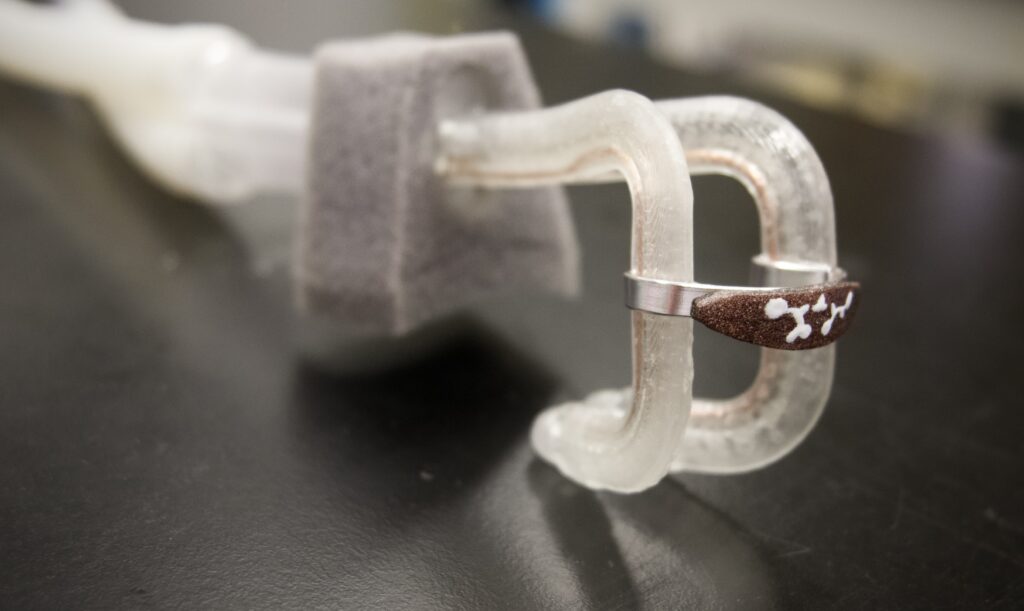
Assembly: Wire was fed through the small lumen in the tubing, allowing the tubing and wire to be bent into their proper shape. Luer locks connected the tubing to the adapter, and the prongs were stretched over the ends of the tube.
Prototype Verification
Our two hallmarks of prototype functionality are sustained air flow delivery and reduction in contact pressure.
Air Flow
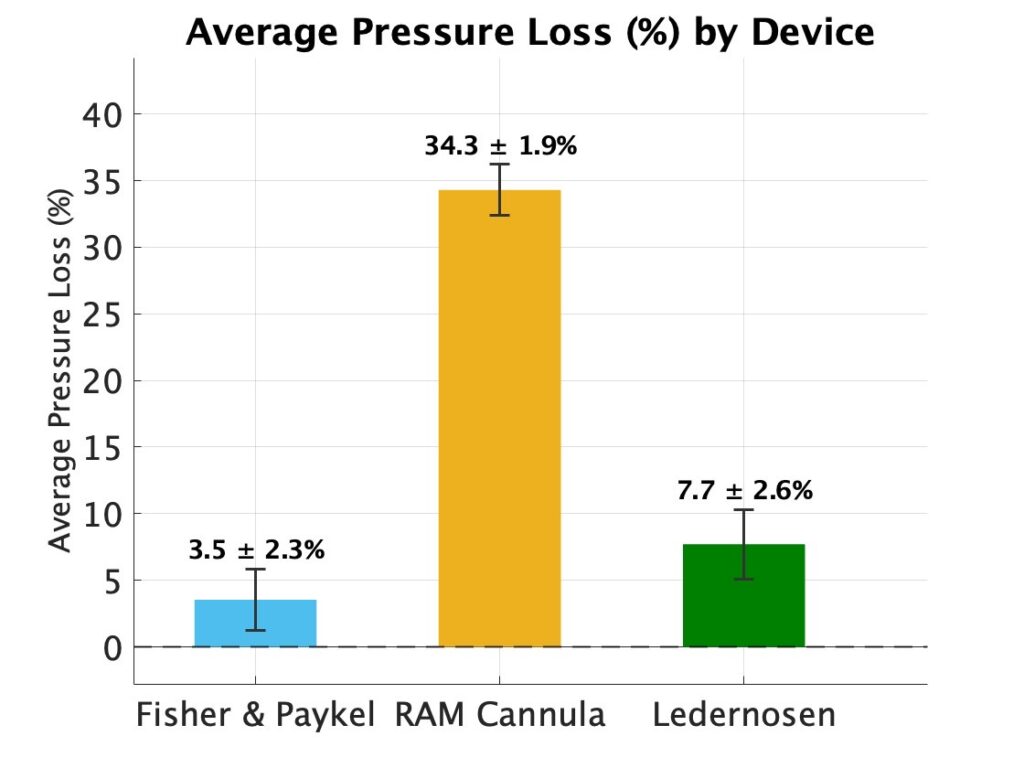
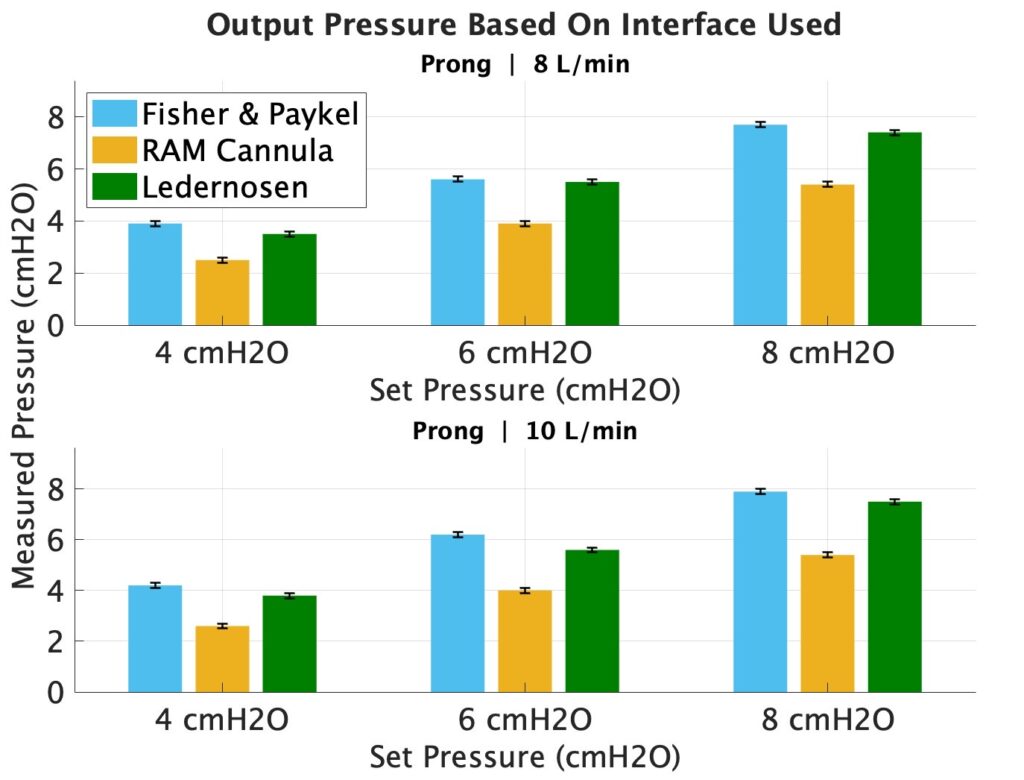
Physical Flow Testing: Ledernosen and predicate devices were connected to bCPAP, and output pressures were measured at varied input bCPAP pressures and air flow rates. Our device maintains pressure comparably to the Fisher & Paykel design, and better than the RAM cannula, meaning our device is sufficiently able to provide air flow and backpressure to support neonatal respiration, satisfying our design metrics (Fig. 1,2).
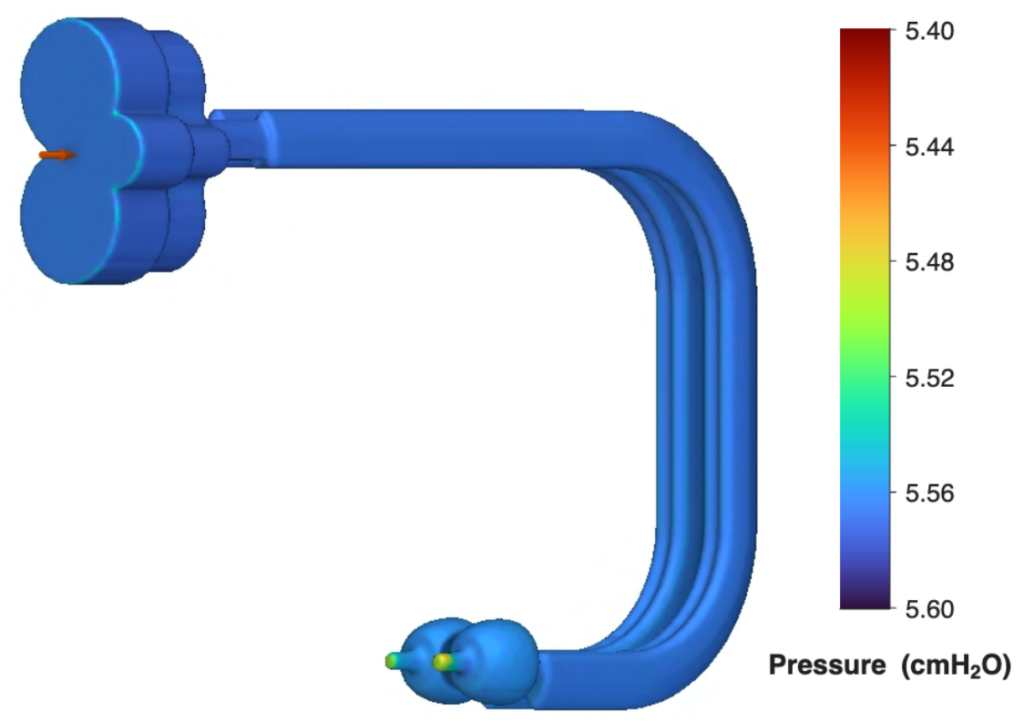
Computational Fluid Dynamics: By importing our CAD design into nTopology, we were able to assess air pressure through all regions of our device. The simulation confirmed negligible loss through the tube lumen, and minimal loss through the prongs (Fig. 3).
Contact Pressure
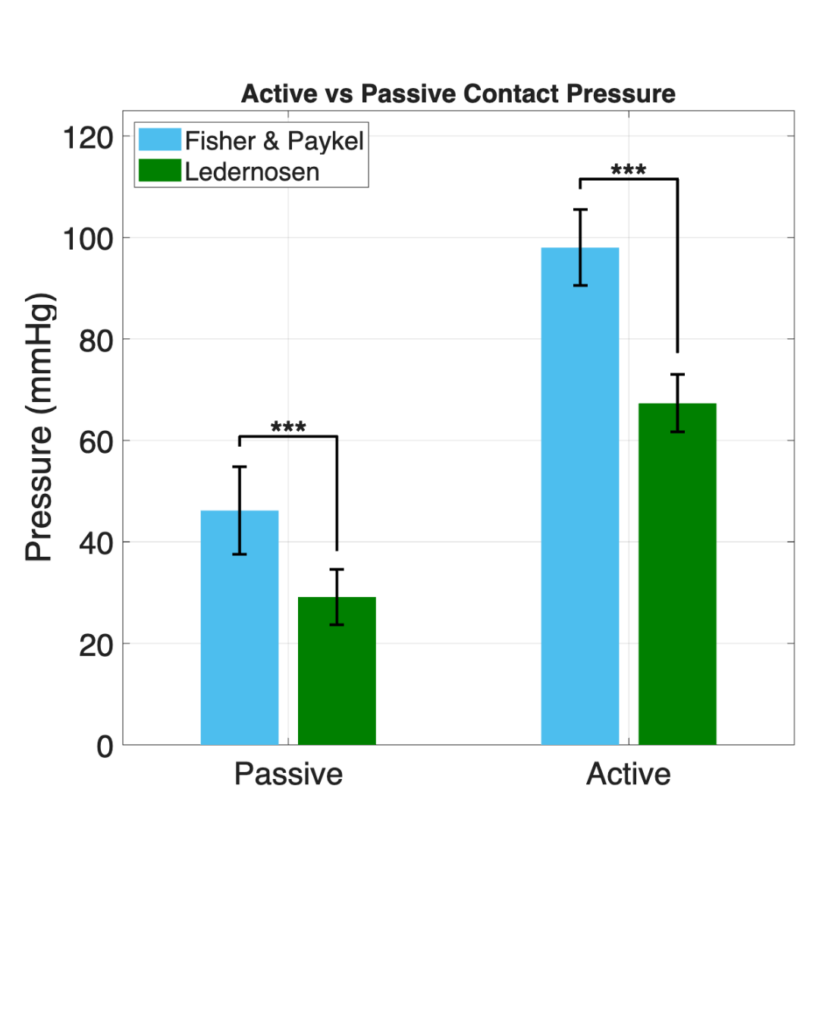
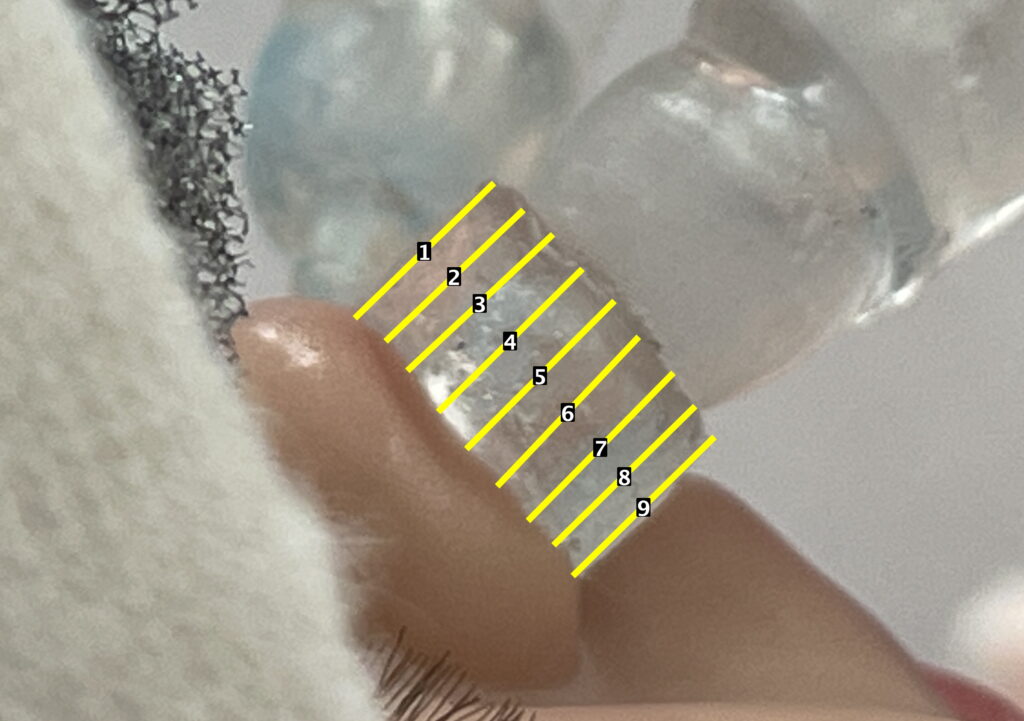
Nare Contact Pressure: Neonatal nare tissue-mimicking pucks were made of PDMS (E = 45kPa), seen in figure 5. An analysis of puck deformation due to passive (resting) and active (applied force) contact was conducted to compare the pressure exerted by the F&P system and Ledernosen on neonatal nares. Results confirmed significant improvement, with our device exerting 36% less passive pressure and 31% less active pressure, and falling within our target design metrics for nare contact pressure.
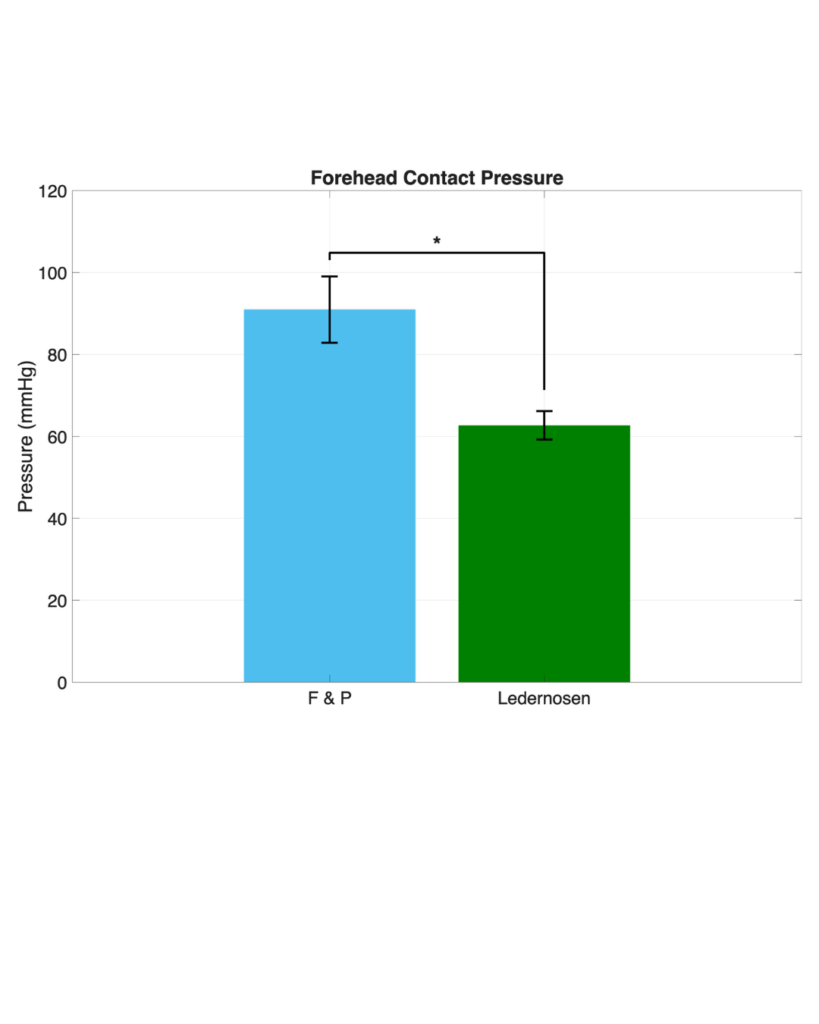
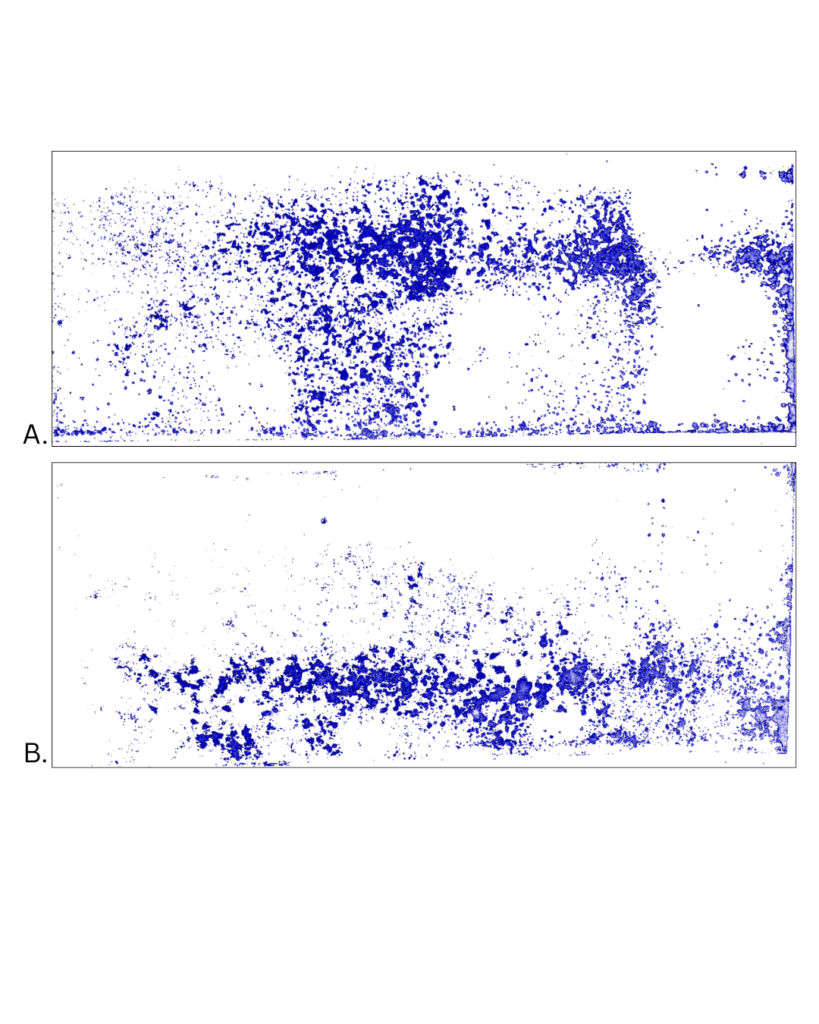
Forehead Contact Pressure: Pressure-sensitive film strips were placed on the manikin, underneath the cap used to secure both systems in place. The tested interfaces were then set up as per standard protocol and left in place for a few seconds before film reaction was assessed. Ledernosen satisfies our target design metrics for forehead pressure.
Future Directions
Regulatory Considerations
• Need FDA Class I or II device approval
• Further conduction of simulations & bench testing
• Clinical testing & approval process
• Market approval
Manufacturing Constraints
• Development of more prong sizing options
• Manufacturing equipment expenses
• Large-scale manufacturing procedures: tube extrusion, wire coating, silicone & plastic injection molding
Use Constraints
• Requirement of Fisher & Paykel bCPAP system availability
• Special clinical training for device administration
Meet the Team

Acknowledgements
We are especially grateful for the guidance of our supervisor Marisol Herrera-Perez, PhD1, professors Scott Seidman, PhD1, and Benjamin Castañeda, PhD1, and project management liason Dinesh Babendala2. This project would not have been possible without the trust of our client Joseph Bliss, MD3, and Rebecca Gillis, RRT3. We are also thankful to Dean G. Johnson, PhD4, for use of his laboratory, and Eric Nauman, PhD5, for his insight. We would like to thank Dr. Greg Gdowski for his insight into airflow and tubing, and Dr. David Foster and Dominic Lippa for their advice with computational fluid dynamics modeling.1,6
1Department of Biomedical Engineering, University of Rochester, 2Center for Medical Technology and Innovation, University of Rochester, 3Golisano Children’s Hospital, 4Department of Nephrology, University of Rochester, School of Medicine and Dentistry, 5University of Cincinnati, Department of Biomedical Engineering, 6Department of Chemical Engineering, University of Rochester.
References
[1] S. Yadav and B. Lee, “Neonatal respiratory distress syndrome,” in StatPearls. Treasure Island, FL, USA: StatPearls Publishing, 2023. Available: https://www.ncbi.nlm.nih.gov/books/NBK560779/
[2] A. D. Zakrajsek, L. Kesterson, M. O. Visscher, V. Narendran, O. S. Hoilett, and E. A. Nauman, “Neonatal Noninvasive Ventilation Nasal Mask Interface Pressure and the Inter-Individual Variation of Mask Placement,” Respir Care, vol. 70, no. 4, pp. 417–426, Apr. 2025, doi: 10.4187/respcare.12217.
[3] C. Fischer, V. Bertelle, J. Hohlfeld, M. Forcada-Guex, C. Stadelmann-Diaw, and J.-F. Tolsa, “Nasal trauma due to continuous positive airway pressure in neonates,” Archives of Disease in Childhood – Fetal and Neonatal Edition, vol. 95, no. 6, pp. F447–F451, Nov. 2010, doi: 10.1136/adc.2009.179416.
[4] “FlexiTrunkTM Nasal CPAP Midline Interface | Fisher & Paykel Healthcare.” Accessed: Feb. 04, 2026. [Online]. Available: https://www.fphcare.com/us/hospital/infant-respiratory/neonates/cpap/flexitrunk-midline/
[5] K. J. Rodriguez, “Diapering for Healthy Skin and Development,” Synova Associates, Oct. 26, 2022. [Online]. Available: https://www.synovaassociates.com/diapering-for-healthy-skin-and-development/ [Accessed: May 5, 2026].
[6] R. Dore et al., “Neonatal blood pressure by birth weight, gestational age, and postnatal age: a systematic review,” Matern Health Neonatol Perinatol, vol. 10, p. 9, May 2024, doi: 10.1186/s40748-024-00180-w.
[7] M. Pawlaczyk, M. Lelonkiewicz, and M. Wieczorowski, “Age-dependent biomechanical properties of the skin,” Postepy Dermatol Alergol, vol. 30, no. 5, pp. 302–306, Oct. 2013, doi: 10.5114/pdia.2013.38359.
[8] X. Feng, G.-Y. Li, A. Ramier, A. M. Eltony, and S.-H. Yun, “In vivo stiffness measurement of epidermis, dermis, and hypodermis using broadband Rayleigh-wave optical coherence elastography,” Acta Biomater, vol. 146, pp. 295–305, Jul. 2022, doi: 10.1016/j.actbio.2022.04.030.